Medicare and the Affordable Care Act
- Preventative Services. The Affordable Care Act also affected Medicare by adding coverage for a "Wellness Visit" and a...
- Wellness Visits. A free yearly “wellness” visit can be used to develop or update a personalized health plan, which is...
- Welcome to Medicare Visits. If you have recently enrolled in Medicare, a “Welcome to Medicare”...
Full Answer
How does the Affordable Care Act affect Medicare?
The Affordable Care Act has changed your Medicare coverage. You Can Get More Care at No Additional Cost Many types of preventive care are now available to you at no additional cost.
What are the cons of the Affordable Care Act?
- People who are younger than age 65
- People in relatively good health
- People who want to shop for affordable doctors, specialists or procedures
- People who want transparency in healthcare costs
What does the Affordable Care Act have to do with Medicare?
Find affordable Medicare plans. The Affordable Care Act (commonly called "Obamacare") requires that all Americans have health insurance that meets minimum essential coverage standards , such as through an employer, veterans benefits, or other source .
What are the reasons for opposing the Affordable Care Act?
The current law provisions include:
- Children can stay on their parent's healthcare plan until age 26.
- No one who is sick or has a medical condition can be denied insurance.
- Companies can no longer charge women more than men.
- Businesses with more than 50 full-time employees must offer health insurance.
How has the Affordable Care Act affect Medicare?
Medicare Premiums and Prescription Drug Costs The ACA closed the Medicare Part D coverage gap, or “doughnut hole,” helping to reduce prescription drug spending. It also increased Part B and D premiums for higher-income beneficiaries. The Bipartisan Budget Act (BBA) of 2018 modified both of these policies.
Does Medicare fall under the Affordable Care Act?
Obamacare's expanded Medicare preventive coverage applies to all Medicare beneficiaries, whether they have Original Medicare or a Medicare Advantage plan.
What did the ACA do for Medicare Advantage?
The ACA reduced payments to Medicare Advantage plans over six years, which brought these payments closer to the average costs of care under the traditional Medicare program. In 2016, federal payments to plans were 2 percent higher than traditional Medicare spending (including quality-based bonus payments to plans).
How is the Affordable Care Act different from Medicare?
Main Differences Between Medicare and the ACA (Obamacare) In the simplest terms, the main difference between understanding Medicare and Obamacare is that Obamacare refers to private health plans available through the Health Insurance Marketplace while Original Medicare is provided through the federal government.
How will ACA repeal affect Medicare?
Dismantling the ACA could thus eliminate those savings and increase Medicare spending by approximately $350 billion over the ten years of 2016- 2025. This would accelerate the insolvency of the Medicare Trust Fund.
How does the Affordable Care Act affect the elderly?
"The ACA expanded access to affordable coverage for adults under 65, increasing coverage for all age groups, races and ethnicities, education levels, and incomes."Under the ACA, older adults' uninsured rate has dropped by a third, indicators of their health and wellness have improved, and they're now protected from ...
How did the ACA expand Medicare?
The ACA gradually reduced costs by restructuring payments to Medicare Advantage, based on the fact that the government was spending more money per enrollee for Medicare Advantage than for Original Medicare.
Is Medicare more expensive than Obamacare?
The average Medicare Part D plan premium in 2021 is $47.59 per month. The average Medicare Supplement Insurance plan premium in 2019 was $125.93 per month. The average Obamacare benchmark premium in 2021 is $452 per month.
What will happen if ACA is repealed?
The health insurance industry would be upended by the elimination of A.C.A. requirements. Insurers in many markets could again deny coverage or charge higher premiums to people with pre-existing medical conditions, and they could charge women higher rates.
How did the ACA reduce Medicare costs?
Cost savings through Medicare Advantage. The ACA gradually reduced costs by restructuring payments to Medicare Advantage, based on the fact that the government was spending more money per enrollee for Medicare Advantage than for Original Medicare. But implementing the cuts has been a bit of an uphill battle.
Why did Medicare enrollment drop?
When the ACA was enacted, there were expectations that Medicare Advantage enrollment would drop because the payment cuts would trigger benefit reductions and premium increases that would drive enrollees away from Medicare Advantage plans.
What is Medicare D subsidy?
When Medicare D was created, it included a provision to provide a subsidy to employers who continued to offer prescription drug coverage to their retirees, as long as the drug covered was at least as good as Medicare D. The subsidy amounts to 28 percent of what the employer spends on retiree drug costs.
How much will Medicare Part B cost in 2021?
In 2021, most Medicare Part B enrollees pay $148.50/month in premiums. But beneficiaries with higher incomes pay additional amounts – up to $504.90 for those with the highest incomes (individuals with income above $500,000, and couples above $750,000). Medicare D premiums are also higher for enrollees with higher incomes.
What percentage of Medicare donut holes are paid?
The issue was addressed immediately by the ACA, which began phasing in coverage adjustments to ensure that enrollees will pay only 25 percent of “donut hole” expenses by 2020, compared to 100 percent in 2010 and before.
How many people will be on Medicare in 2021?
However, those concerns have turned out to be unfounded. In 2021, there were 26 million Medicare Advantage enrollees, and enrollment in Advantage plans had been steadily growing since 2004.; Medicare Advantage now accounts for 42% of all Medicare beneficiaries. That’s up from 24% in 2010, which is the year the ACA was enacted (overall Medicare enrollment has been growing sharply as the Baby Boomer population ages into Medicare, but Medicare Advantage enrollment is growing at an even faster pace).
What is the medical loss ratio for Medicare Advantage?
This is the same medical loss ratio that was imposed on the private large group health insurance market starting in 2011, and most Medicare Advantage plans were already conforming to this requirement; in 2011, the average medical loss ratio for Medicare Advantage plans was 86.3%. The medical loss ratio rules remain in effect, but starting in 2019, the federal government has reduced the reporting burden for Medicare Advantage insurers.
How much will Medicare pay in 2020?
For instance, if your adjusted gross income in 2018 was $87,000 to $109,000 a year ($174,000 to $218,000 for a couple), you pay $202.40 for your Part B coverage in 2020.
When is the open enrollment period for Medicare Advantage?
That’s why it’s important to shop for plans each year during the Open Enrollment Period from October 15 to December 7 each year.
Do you pay higher premiums if you have a high income?
Have a High-Income? You'll Pay Higher Premiums
Can Medicare Advantage plan change from year to year?
If you have a Medicare Advantage plan, which is also known as Medicare Part C , from a private company, your coverage may change from year to year. Unlike traditional Medicare, if you are in a Medicare Advantage plan you must get your care from a network provider. The Affordable Care Act says that your insurance company will get a bonus ...
What is the impact of the Affordable Care Act on Medicare?
Among other benefits, the Affordable Care Act (ACA) helps individuals on Medicare to save money with preventative care and brand-name drugs. Starting in January 2014, Medicare began covering many preventative services with no out-of-pocket expense. This coverage includes an annual wellness visit ...
What is the Medicare donut hole?
This refers to a temporary limit on prescription drug coverage, where the policy holder needs to pay a higher percentage of his or her medications after reaching this limit.
When will Medicare Part D donut hole close?
Medicare recipients will see some changes in their out-of-pocket expenses as the Medicare Part D donut hole is incrementally lowered to finally “close” in the year 2020. At that time, Medicare recipients will pay 25 percent of the drug cost.
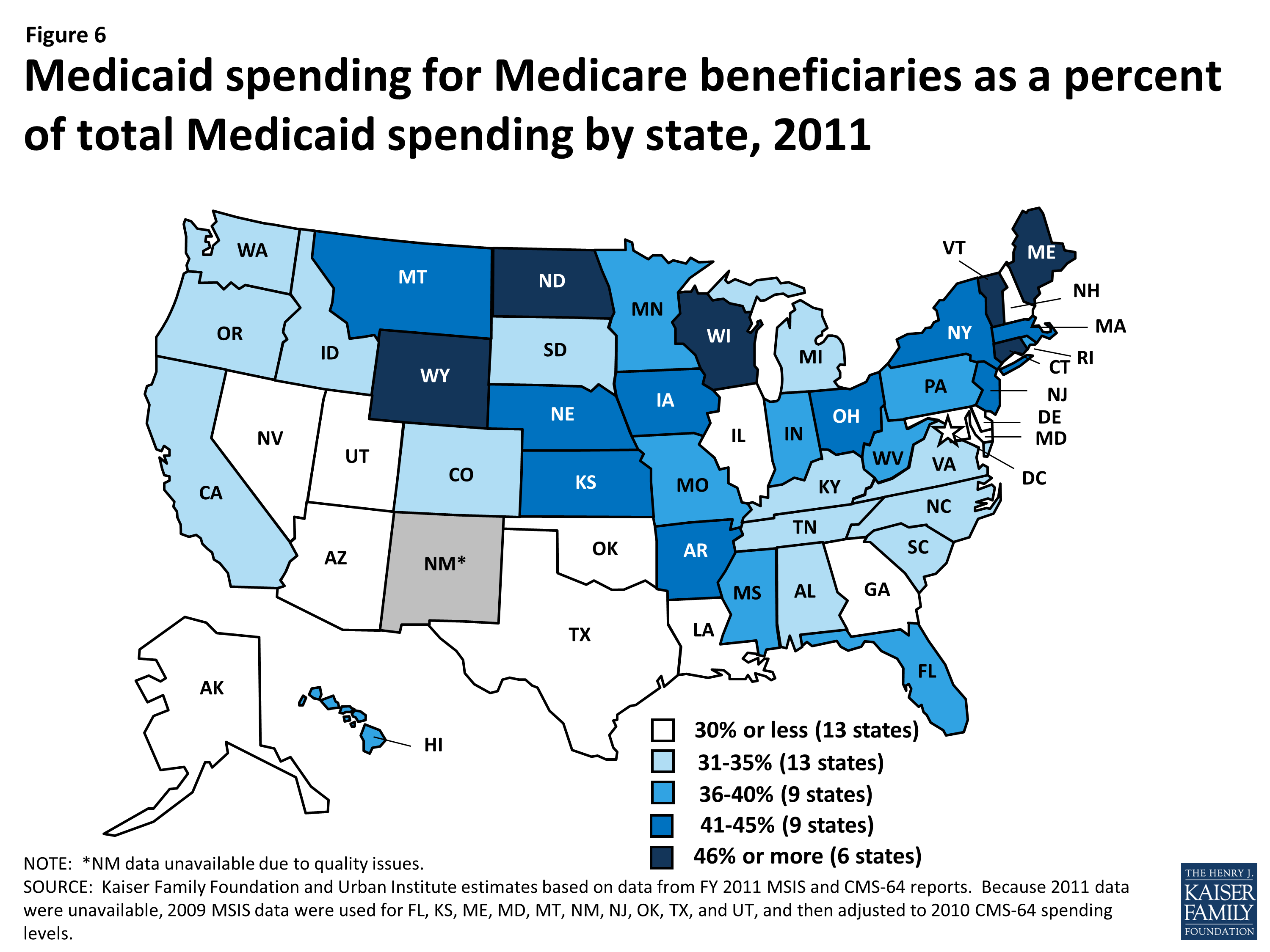
Is Medicare considered a dual insurance?
If you are “Dual Eligible,” generally Medicare would be billed first or considered your primary insurance, and then Medicaid would be billed for the balance acting as a secondary insurance. Please contact your local Department of Human Resources to determine if you qualify.
How does the Medicare law affect hospitals?
It also penalizes hospitals with too many readmissions of Medicare patients who have heart attacks , heart failure or pneumonia within 30 days of a hospital stay.
How much will Medicare be reduced?
The nonpartisan Congressional Budget Office estimated that Medicare spending would be reduced by $716 billion over 10 years, mainly because the law puts the brakes on annual increases in Medicare reimbursement for Medicare Advantage, hospital costs, home health services, hospices and skilled nursing services.
How many states have Medicare cut doctors?
The American Medical Association says that in at least 11 states, Medicare Advantage plans have cut thousands of physicians. Critics worry that more doctors may stop taking Medicare patients or that patients will face lengthy waits for appointments or other changes.
How much less will Medicare get in 2022?
Other cuts include $66 billion less for home health, $39 billion less for skilled nursing services and $17 billion less for hospice care — all by 2022. Medicare costs will still grow, just more slowly than they would without the ACA. But some experts predict that beneficiaries will feel ...
What is Medicare Advantage?
About three in 10 Medicare beneficiaries are enrolled in Medicare Advantage options, which are premium insurance plans that often include dental, vision and drug insurance. These plans have been subsidized by the federal government for years. The ACA is simply aiming to equalize costs, according to its proponents.
Did Medicare change before the law?
Insurers changed Medicare Advantage plans before the law, and they're still changing them, he says. "Overall, seniors are not paying that much more, and more people are still enrolling in Medicare Advantage plans," says Gruber, who advised the Obama administration on the ACA.
Is the ACA good for Medicare?
But Henry J. Aaron of the Brookings Institution, a liberal think tank, insists that "the ACA is unalloyed good news" for Medicare beneficiaries because it improves the financial health of Medicare Part A, the hospital insurance program.
How long did the Affordable Care Act last?
While the Affordable Care Act (ACA) increased insurance coverage and access to care after 1 (2014) or 2 (2014-2015) postreform years, the existing causally interpretable evidence suggests that effects on self-assessed health outcomes were not as clear after 2 years.
What effect did the third year of the health insurance policy have on the health insurance coverage?
We find that gains in health insurance coverage and access to care from the policy continued to increase, while an improvement in the probability of reporting excellent health emerged in the third year, with the effect being largely driven by the non-Medicaid expansions components of the policy .
Why were people over 64 excluded from the ACA?
Individuals older than 64 years were excluded because the ACA was not intended to affect their health care coverage. Our sample starts in 2011 because this is the first year in which the BRFSS included cell phones in its sampling frame. A 2011-2016 sample period gives us 3 years of pretreatment data and 3 years of posttreatment data.
How many variables are used in the outcome of a health care study?
We utilize 9 outcome variables. The first 3 relate to access to care: indicators for any health insurance coverage, having a primary care doctor, and having any care needed but foregone because of cost in the past 12 months. The remaining outcomes relate to self-assessed health status. These include dummy variables for whether overall health is good or better (ie good, very good, or excellent), very good or excellent, and excellent, as well as days of the last 30 not in good mental health, not in good physical health, and with health-related functional limitations. Subjective self-assessed health variables such as these have been shown to be correlated with objective measures of health, including mortality.31-33
Which states have expanded Medicaid?
Pennsylvania, Indiana, and Alaska expanded Medicaid in January, February, and September of 2015, respectively. Montana and Louisiana expanded Medicaid in January and July of 2016, respectively. States are classified as part of the Medicaid expansion treatment group beginning the month/year of their expansion.
Does the ACA affect mental health?
With respect to self-assessed health, we find that the ACA increased the probability of reporting excellent health and reduced days in poor mental health. In contrast, a recent article with only 2 posttreatment years found no evidence of gains in these outcomes despite also using BRFSS data and the same identification strategy.18The emergence of an impact on the probability of having excellent self-assessed health appears particularly gradual, as the effect of the full ACA was small and insignificant in 2014, 1.9 percentage points in 2015, and 2.7 percentage points in 2016. Improvements in self-assessed health at lower points of the distribution also emerge in 2016. Most of these gains appear to come from the non-Medicaid-expansion components of the law.
How does the ACA affect health care?
The Patient Protection and Affordable Care Act (ACA) expands access to health insurance in the United States , and, to date, an estimated 20 million previously uninsured individuals have gained coverage. Understanding the law’s impact on coverage, access, utilization, and health outcomes, especially among low-income populations, is critical to informing ongoing debates about its effectiveness and implementation. Early findings indicate that there have been significant reductions in the rate of uninsurance among the poor and among those who live in Medicaid expansion states. In addition, the law has been associated with increased health care access, affordability, and use of preventive and outpatient services among low-income populations, though impacts on inpatient utilization and health outcomes have been less conclusive. Although these early findings are generally consistent with past coverage expansions, continued monitoring of these domains is essential to understand the long-term impact of the law for underserved populations.
What are the effects of pre-ACA coverage?
Pre-ACA insurance expansions have largely demonstrated improved access to care for low-income populations. For example, the Massachusetts health reform was associated with significant reductions in forgone or delayed care and improvements in access to a personal doctor and usual source of care among adults overall (46, 54, 56, 58, 72, 88) and, in particular, for subgroups targeted by the ACA, such as low-income and childless adults (54, 56, 58). With regard to affordability, the Medicaid expansion in Oregon diminished financial hardship from medical costs, markedly reducing catastrophic OOP expenditures (5, 35, 98). In addition, other states that expanded public insurance prior to the ACA demonstrated improvements in access and affordability among low-income adults (62, 82) and children (33, 44) across comparable measures. More recently, the California LIHP waiver project found large reductions in the likelihood of any family OOP health care spending but did not detect significant differences in access to care, which may be explained by a well-established safety net in the state prior to program implementation (38). One ongoing concern about expanding coverage is that increased demand for services by newly insured individuals may limit access to care, but evidence from prior expansions does not appear to sufficiently support this hypothesis (67).
How does the reliance on the ACA affect health insurance?
Despite the availability of subsidies and cost-sharing reductions, the reliance of the ACA on health insurance exchanges may both increase access to health insurance and simultaneously pose unintended barriers to access, particularly for low-income populations. These barriers can arise in two ways. The most publicized method is through the creation of narrow networks, where insurers offer plans and policies with fewer doctors and hospitals in an effort to keep premiums as competitive as possible. Whether narrow networks create actual, rather than perceived, barriers to care has not been well established yet through research. Nevertheless, the existence of narrow networks has created the perception that exchange-based QHPs are limiting access to a greater extent than did pre-ACA policies, despite the absence of adequate baseline data from pre-ACA years.
What is the coverage gap?
Approximately 9% of the remaining uninsured (almost 3 million Americans) fall into what is known as the “coverage gap.” This group represents poor, uninsured adults who reside in the 19 non–Medicaid expansion states whose income is above the state’s threshold for Medicaid eligibility but less than the 100% threshold for Marketplace subsidy eligibility. Also included are childless adults who were not previously eligible for Medicaid. Almost 90% of all adults in the coverage gap live in the South, half in either Texas or Florida, which aligns with this region’s high uninsurance rates, limited Medicaid eligibility, and low uptake of Medicaid expansion (37). Consistent with demographic characteristics and policies excluding nondisabled adults in states that did not expand Medicaid, African Americans and childless adults also account for a disproportionate share of individuals in the coverage gap (37). If all current nonexpansion states opted to expand Medicaid, 5.2 million currently uninsured adults would gain coverage: 2.9 million who are in the coverage gap, 0.5 million who are already eligible for Medicaid though alternate pathways, and an additional 1.8 million who are presently eligible for Marketplace subsidies with incomes from 100% FPL to 138% FPL yet did not enroll (37). Because a substantial portion of the remaining uninsured are either eligible for coverage or fall in the coverage gap, the law’s potential impact on the poor has not yet been fully realized.
How effective is Medicaid expansion?
The expansion of Medicaid has been particularly effective in states that took advantage of the opportunity for early Medicaid expansion allowed under the ACA. Between 2010 and 2014, six states (California, Colorado, Connecticut, Minnesota, New Jersey, Washington) and the District of Columbia extended Medicaid eligibility for low-income adults through the early Medicaid expansion option or the Section 1115 waiver process (18). In California, the LIHP significantly increased coverage by 7.3 percentage points for poor adults (up to 138% FPL) within the first two years (38). Similarly, one year after early expansion, Medicaid coverage increased significantly in Connecticut (4.9 percentage points) and modestly in Washington, DC (3.7 percentage points) among low-income childless adults—a key subpopulation targeted by Medicaid expansion (86). Trends in coverage gains in these early expansions echoed those of the Massachusetts health reform, which was associated with an estimated 18.4-percentage-point increase in coverage among low-income adults and even larger gains among low-income childless adults (54). Though these expansions were implemented prior to the ACA, their positive findings inform potential coverage gains for the poor under the ACA.
What is the goal of increased coverage eligibility and affordability?
An important goal of increased coverage eligibility and affordability is to increase access to adequate health care services for the poor. As a result, the ACA’s impact on access to high-quality health care has been evaluated across multiple dimensions, including access to a doctor, having a usual source of care, timeliness of care, affordability, and access to medications and preventive, primary, and specialty care.
Does the ACA expand Medicaid?
In summary, early evidence following ACA implementation has demonstrated significant progress toward its goal of expanding coverage for millions of low-income individuals who would have otherwise remained uninsured. Not all individuals equally experience the potential benefits of the law, however, and disparities have developed on the basis of state decisions regarding whether to expand Medicaid.
How did the ACA increase the number of Americans with health insurance?
Beyond the Medicaid expansion, the ACA sought to increase the number of Americans with health insurance by providing new premium tax credits for the purchase of private health insurance and made a number of reforms to the private insurance market, such as eliminating preexisting condition exclusions and establishing annual limits on out-of-pocket costs. The law also allowed young adults to remain on their parents’ insurance plans up to age 26 and required most individuals to secure minimum essential coverage. 2
When did the Supreme Court rule on Medicaid expansion?
Originally a requirement, the June 2012 Supreme Court ruling in National Federation of Independent Business v. Sebelius effectively made the Medicaid expansion an option. To date, almost three-quarters of states have opted to expand.
What is the minimum FPL for Medicaid?
The ACA also aligned states’ minimum Medicaid eligibility threshold for children at 133 percent FPL, requiring some states to shift older children from separate CHIP programs into Medicaid. Prior to the ACA, the mandatory eligibility levels for children in Medicaid differed by age: States were required to cover infants and children between ...
What is the ACA 111-148?
The Patient Protection and Affordable Care Act (ACA, P.L. 111-148, as amended) made a number of changes to Medicaid. Perhaps the most widely discussed is the expansion of eligibility to adults with incomes up to 133 percent of the federal poverty level (FPL). 1
Does the ACA require a single application for Medicaid?
The ACA also included provisions to streamline eligibility, enrollment, and renewal processes, for example, by requiring a single application for Medicaid, CHIP, and subsidized exchange coverage. In part due to these changes, enrollment and spending in Medicaid has increased in all states, regardless of whether the state expanded coverage ...